
20 years TauroLock™
Revisiting milestones in research
As of 2024, TauroLock™ has been on the market for two decades. At the time of the initial launch in 2004, the first publications on our products were well underway. A lot has happened since then – from clinical trials to recommendations in national and international guidelines. To give you an overview, here’s a timeline of the most important literature to date.
TauroLock™ solutions in dialysis
2001
A “new antimicrobial lock solution”
Three years before TauroLock™ entered the market, Sodemann et al. published “the first study using an antimicrobial catheter locking solution in a large number of patients”. [1] Overall, this real-world study included 70 patients dependent on haemodialysis. After one year of using the TauroLock™ formula on a regular basis, more than 60 % of patients had developed zero infections. The rate of normalised bloodstream infections amounted to 0.29 per 1,000 catheter days. [1]
2002
A forecast of “crucial advance”
Next, Quarello et al. offered a glimpse into the future of haemodialysis treatment. The authors had taken a closer look at existing findings on the use of lock solutions with 1.35 % taurolidine and 4 % citrate. Quarello et al. concluded their review by stating that “clinical results with taurolidine-based lock solutions appear to be a crucial advance” in the prevention of catheter-related infections – but still “await further confirmation from ongoing clinical trials”. [2]
2003
Introducing a novel lock solution
Following the “promising results” [2] shared by Quarello et al., Allon provided further evidence for the efficacy of TauroLock™ (referred to as an “investigational preparation” [3] at the time). He found that compared to heparin, the formula of 1.35 % taurolidine + 4 % citrate “dramatically reduces the frequency of catheter-related bacteremia among patients undergoing hemodialysis”. [3] However, Allon also reported an “increased requirement for thrombolytic interventions to maintain catheter patency”. [3] This observation reiterated the necessity of specialised lock solutions to meet the individual needs of each patient. Hence why we developed two product variants with heparin later on: TauroLock™-HEP100 and TauroLock™-HEP500.
2004
The first clinical trial
In the same year TauroLock™ was launched, Betjes et al. published the first randomised trial demonstrating its antimicrobial efficacy. The authors tested the use of our product in comparison with heparin as a lock solution in dialysis patients. They found that TauroLock™ “is effective and safe for the prevention of CRS [catheter-related sepsis]” and “may lead to a sizeable reduction in CRS incidence, even in a dialysis centre where CRS incidence is already low using heparin”. [4]
2008
Proven cost effectiveness
Four years onwards, another clinical study attested to the efficacy of TauroLock™ in haemodialysis. Taylor et al. observed a decrease of catheter-related infections by 88.5 % over a period of six months – from 5.2 down to 0.6 infections per 1,000 catheter days. They also pointed out that the use of TauroLock™ led to considerable cost savings: €10 for each catheter day, even after the expenses for the product itself had been included. [5] Similar to Quarello et al., Taylor et al. reported that some patients experienced patency issues. They managed to solve this problem by adding a “small amount” (0.6 ml of 5,000 IU/ml) heparin to the lock solution – thus paving the way for TauroLock™-HEP500 in haemodialysis. [5]

2010
TauroLock™-HEP500 moving into focus
In 2010, a randomised controlled trial once again suggested that the key to effective lock solutions lies in a combination of different active ingredients. Solomon et al. echoed the findings of Taylor et al. [5] and Allon [3]: In their study, TauroLock™ (i.e. 1.35 % taurolidine and 4 % citrate) was associated with a lower rate of bacteraemia, but also a higher rate of thrombosis. The authors therefore pointed to the need for a “formulation with better anticoagulant properties” in haemodialysis. [6] At the time, this formulation was already available in another product variant that we had added to our portfolio in 2007: TauroLock™-HEP500 with 1.35 % taurolidine, 4 % citrate, and 500 IU/ml heparin.
2017
Putting TauroLock™-U25.000 on the map
TauroLock™-HEP500 was not the last addition to our portfolio. For a particularly strong prophylaxis against thrombosis, we developed TauroLock™-U25.000: A lock solution based on taurolidine and low concentrated citrate, along with 25,000 units urokinase. In 2017, Al-Ali et al. published a randomised controlled study on what has come to be known as the 2+1 protocol: TauroLock™-HEP500 twice a week, plus TauroLock™-U25.000 once a week. They found that this regimen “led to reduced incidence of catheter exchanges and decreased the need for emergency thrombolysis”. [7] TauroLock™-U25.000 was therefore deemed “a safe and effective tunneled dialysis catheter lock solution”. [7]

2018
Saving costs with the 2+1 protocol
Following the publication of Al-Ali et al. (7), another randomised controlled trial provided strong arguments for the combined use of TauroLock™-HEP500 and TauroLock™-U25.000: Winnicki et al. reported that the 2+1 protocol led to significantly lower rates of catheter-related complications in haemodialysis patients (compared to 4 % citrate). This resulted in a 43 % reduction of expenses per patient/year. The authors concluded that the TauroLock™ 2+1 protocol was “overall more cost-efficient". [8]
TauroLock™ solutions in parenteral nutrition
1998
Discovering an “effective and safe antimicrobial agent”
Toward the end of the 20th century, Jurewitsch et al. published a case report on the use of taurolidine in parenteral nutrition. [9] Albeit anecdotal, their findings paved the way for future research: The study subject was a 29-year old patient who received home parenteral nutrition (HPN) due to short bowel syndrom. He had been admitted 18 times because of catheter-related bloodstream infections (CRBSI) over the course of nine years. Ten months before the last infection, the patient started locking his catheter with 2 % taurolidine after each HPN session. Two years later, the CRBSI rate had decreased from 8.5 to 1.5 per 1,000 catheter days. The authours concluded that “taurolidine may prove to be an effective and safe lock solution for the prevention of recurrent [CRBSIs]”. [9]
2012
Lock your line, every time
It took more than a decade until the next significant publication on taurolidine in parenteral nutrition: Touré et al. investigated the efficacy of TauroLock™ as secondary prevention in high-risk HPN patients. [10] In particular, they compared the results of locking the catheter once a week vs. locking it after every single treatment (i.e. daily). The outcome was unequivocal: Among patients who received TauroLock™ on a weekly basis, the CRBSI rate decreased from 4.8 to 1.37 per 1,000 catheter days. Daily use after each treatment, on the other hand, resulted in a decrease from 8.61 to 0.78 per 1,000 catheter days. [10] Hence why we always recommend locking your line every time.
2012
A safe solution for paediatric patients
Only a few months later, Chu et al. also published a study on the use of TauroLock™ in HPN. [11] They compared it against heparin in 19 paediatric patients over a period of up to 33 months. In the end, TauroLock™ had led to a “reduced incidence of CRBSI [catheter-related bloodstream infections] ... without the risk of inducing bacterial resistance or any other adverse effects”. [11] The authors therefore suggested a recommendation of TauroLock™ as secondary prevention in all children dependent on PN with a history of septicemia.
2018
Reconsidering secondary prevention
The findings of Chu et al. were substantiated six years later, when Lambe et al. published a study on TauroLock™ in children with intestinal failure. [12] Used as secondary prevention, it reduced the CRBSI rate from 4.16 to 0.25 per 1,000 catheter days with “no sign of any adverse event”. [12] But the authors made another significant observation: A large proportion of patients (i.e. children with immune deficiency or children with definitive intestinal failure and risk factors for nutritional failure) were considered “good candidates” [12] for primary prevention with TauroLock™. According to the authors, a single CRBSI might otherwise impair the efficacy of lock solutions used afterwards. [12]

2018
Recommendation for paediatric patients
In line with the positive outcomes reported by Chu and Lambe et al., the ESPGHAN/ESPEN/ESPR/CSP issued a new recommendation in 2018. According to the expert panel, “[t]aurolidine is effective in preventing CRBSI and should be used during long term catheter use” in paediatric parenteral nutrition. [3]
2019
(Cost-)effective protection for small children
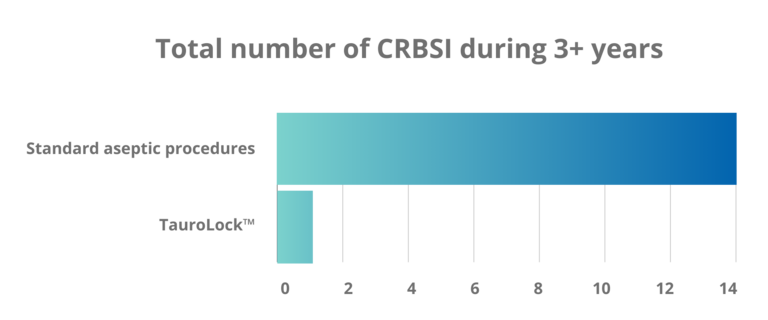
Continuing the research on TauroLock™ in paediatric patients, Lyszkowska et al. focused on children under two years of age. [14] In this case, the catheter lock regimen was not limited to secondary prevention: All 86 patients either underwent “standard aseptic procedures” [14] or received TauroLock™ for the duration of the trial. In the end, Lyszwkowska et al. reported a significant difference between both groups: 14.3 infections per 1,000 catheter days without TauroLock™ and 1.06 with TauroLock™. They also found that treating a catheter-related infection was 28.7 times more expensive than prophylactic catheter locking. The authors therefore deemed TauroLock™ “a safe and cost-effective method for the prevention of CRIs in very young children”. [14]
2020
From heparin to TauroLock™-HEP100
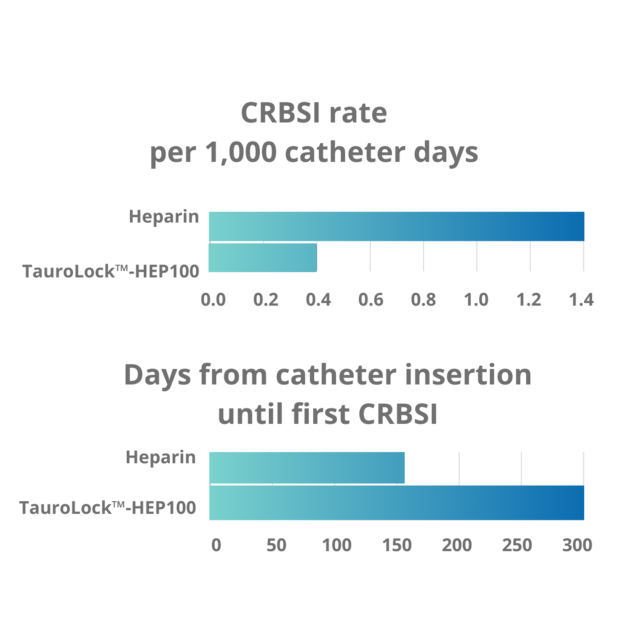
TauroLock™-HEP100 was developed for patients who have previously relied on heparin to maintain patency. In 2020, a longitudinal cohort series confirmed the sustained efficacy of this product: Leiberman et al. examined data from 169 patients in HPN between 1998 and 2017. [15] Among the group of patients who switched from heparin to TauroLock™-HEP100, the CRBSI rate decreased from 2.36 to 0.3 per 1,000 catheter days. The authors concluded their study by recommending the use of TauroLock™-HEP100 “in patients who have recurrent infections”. [15]
2020
Recommendation in ESPEN guideline
In the same year Leiberman et al. published their longitudinal study, the ESPEN guideline on HPN made a significant adjustment. Recommendation no. 34 now states: “As an additional strategy to prevent CRBSIs, taurolidine locking should be used because of its favorable safety and cost profile”. [16]

2023
Making the case for primary prevention
A multi-national ESPEN survey, published in 2023, confirmed that taurolidine has become the expert’s choice for catheter locking: 80 % of all included centres used preventive lock solutions after the first CRBSI, with 84 % of these based on taurolidine. [17] While the survey signaled an important advance in standard practices, it still left room for improvement. The question remains: Why stick to secondary prevention when you could use lock solutions with a “favorable safety and cost profile” from the very start?
TauroLock™ solutions in oncology
2012
Zero colonisation with immediate locking
After eight years of TauroLock™ on the market, the first randomised controlled trial on its efficacy in paediatric cancer patients was published: Dümichen et al. observed 71 children and adolescents to compare two types of lock solutions. [18] They reported a CRBSI rate of 0.3 per 1,000 catheter days in patients receiving TauroLock™ – vs. 1.3 with heparin. Another notable observation: The longer a catheter was used without any locking, the higher the risk of catheter colonisation. Catheters locked immediately with TauroLock™, on the other hand, remained free from colonisation. [18] Once again, a case in point for the benefits of primary prevention.
2013
Significant improvements for children with cancer
The next randomised trial in paediatric oncology followed one year after the publication of Dümichen et al. Again, TauroLock™ was compared against heparin and again, the difference was clear: 0.4 CRBSI per 1,000 catheter days with TauroLock™ vs. 1.4 with heparin. [19] The authors reported similar numbers for the rate of total bloodstream infections per 1,000 catheter days: 1.2 with TauroLock™ vs. 2.5 with heparin. Overall, Handrup et al. concluded that TauroLock™ “significantly reduces catheter-related bloodstream infections in children with cancer”. [19]
2020
A “highly successful” lock therapy
Research on lock solutions in paediatric cancer patients continued: In 2020, Chong et al. published a study that included 33 children with central-venous catheters (CVC). [20] The use of TauroLock™ proved “highly successful” [20]: Among the 20 children who carried a CVC due to a haematological/oncological diagnosis, the rate of central-line-associated bloodstream infections (CLBASI) decreased from 16.55 to 2.81 per 1,000 catheter days. Chong et al. consequently found the solution to be an “effective catheter lock therapy to reduce CLABSI rates in paediatric patients on long-term CVCs”. [20]
TauroLock™ solutions in intensive care
2023
Effective prevention for the most vulnerable patients
Besides dialysis, parenteral nutrition, and oncology, one other field of application has been moving into focus: Antimicrobial lock solutions can turn into a literal lifeline for patients at intensive care untis (ICU). The first significant publication in this regard came out in 2023: Savarese et al. conducted a retrospective study on taurolidine in critical neonates. [21] Their venous access devices (VAD) were locked with 2 % taurolidine, either before or after the first infection had occurred. When used as secondary prevention (along with antibiotic treatment), taurolidine proved effective in 18 of 21 cases. When used as primary prevention, taurolidine led to a complete absence of catheter-related infections. [21]
References
- Sodemann et al. Two years' experience with Dialock and CLS (a new antimicrobial lock solution). Blood Purif 2001. DOI: 10.1159/000046950
- Quarello et al. Prevention of hemodialysis catheter-related bloodstream infection using an antimicrobial lock. Blood Purif 2002. DOI: 10.1159/000046990
- Allon. Prophylaxis against dialysis catheter-related bacteremia with a novel antimicrobial lock solution. Clin Infect Dis 2003. DOI: 10.1086/375234
- Betjes et al. Prevention of dialysis catheter-related sepsis with a citrate–taurolidine-containing lock solution. Nephrol Dial Transplant 2004. DOI: 10.1093/ndt/gfh014
- Taylor et al. A new haemodialysis catheter-locking agent reduces infections in haemodialysis patients. J Ren Care 2008. DOI: 10.1111/j.1755-6686.2008.00027.x
- Solomon et al. A randomized double-blind controlled trial of taurolidine-citrate catheter locks for the prevention of bacteremia in patients treated with hemodialysis. Am J Kidney Dis 2010. DOI: 10.1053/j.ajkd.2009.11.025
- Al-Ali et al. Safety and efficacy of taurolidine/urokinase versus taurolidine/heparin as a tunneled catheter lock solution in hemodialysis patients: a prospective, randomized, controlled study. Nephrol Dial Transplant 2018. DOI: 10.1093/ndt/gfx187
- Winnicki et al. Taurolidine-based catheter lock regimen significantly reduces overall costs, infection, and dysfunction rates of tunneled hemodialysis catheters. Kidney Int 2018. DOI: 10.1016/j.kint.2017.06.026
- Jurewitsch et al. Taurolidine 2% as an antimicrobial lock solution for prevention of recurrent catheter-related bloodstream infections. JPEN J Parenter Enteral Nutr 1998. DOI: 10.1177/0148607198022004242
- Touré et al. Taurolidine lock solution in the secondary prevention of central venous catheter-associated bloodstream infection in home parenteral nutrition patients. Clin Nutr 2012. DOI: 10.1016/j.clnu.2012.01.001
- Chu et al. Significant reduction in central venous catheter-related bloodstream infections in children on HPN after starting treatment with taurolidine line lock. J Pediatr Gastroenterol Nutr 2012. DOI: 10.1097/MPG.0b013e31825bb0ae
- Lambe et al. Strategies to Reduce Catheter-Related Bloodstream Infections in Pediatric Patients Receiving Home Parenteral Nutrition: The Efficacy of
Taurolidine-Citrate Prophylactic-Locking. JPEN J Parenter Enteral Nutr 2018. DOI: 10.1002/jpen.1043 - Kolaček et al. / ESPGHAN/ESPEN/ESPR/CSPEN working group on pediatric parenteral nutrition. ESPGHAN/ESPEN/ESPR/CSPEN guidelines on pediatric parenteral nutrition: Venous access. Clin Nutr. 2018. DOI: 10.1016/j.clnu.2018.06.952
- Lyszkowska et al. Effects of prophylactic use of taurolidine-citrate lock on the number of catheter-related infections in children under 2 years of age undergoing surgery. J Hosp Infect 2019. DOI: 10.1016/j.jhin.2019.04.022
- Leiberman et al. The incidence and management of complications of venous access in home parenteral nutrition (HPN): A 19 year longitudinal cohort series. Clin Nutr ESPEN 2020. DOI: 10.1016/j.clnesp.2020.03.025
- Pironi et al. ESPEN guideline on home parenteral nutrition. Clin Nutr 2020. DOI: 10.1016/j.clnu.2020.03.005
- Joly et al. A multi-national survey of experience and attitudes towards managing catheter related blood stream infections for home parenteral nutrition. Clin Nutr ESPEN 2023. DOI: 10.1016/j.clnesp.2023.06.032
- Dümichen et al. Randomized controlled trial of taurolidine citrate versus heparin as catheter lock solution in paediatric patients with haematological malignancies. J Hosp Infect 2012. DOI: 10.1016/j.jhin.2012.01.003
- Handrup et al. Central venous catheters and catheter locks in children with cancer: a prospective randomized trial of taurolidine versus heparin. Pediatr Blood Cancer 2013 DOI: 10.1002/pbc.24482
- Chong et al. Taurolidine-citrate lock solution for the prevention of central line-associated bloodstream infection in paediatric haematology-oncology and gastrointestinal failure patients with high baseline central-line associated bloodstream infection rates. J Paediatr Child Health 2020. DOI: 10.1111/jpc.14506
- Savarese et al. Use of 2% taurolidine lock solution for treatment and prevention of catheter-related bloodstream infections in neonates: a feasibility study. J Hosp Infect 2023. DOI: 10.1016/j.jhin.2023.11.003